Cycloid psychosis
acute psychosis
The relationship of bulimia and anorexia nervosa with bipolar disorder
Bulimia nervosa in atypical depression
作り物に反応する脳
脳は現実そのものを認知しているのではないのだと
改めて納得する
作り物は本物の薄められたもの
というのがなんとなく正しいような気がするが
人間の脳は果てしなく騙される
脳を最大限に効率良く騙すことが追求されるので
それは脳研究そのものに近くなる
脳にとっては作り物のほうが効率がよく外れがない
しかしDNAが求めているのはそれではない
そこが重要である
福ネコ トキソプラズマ ドーパミン
昔からネコは、幸運や商売繁盛を呼び込む「福ネコ」としてかわいがられ、魔除けや疫病払いの効果があるとされてきた。一方で、「妊婦がネコを触ると流産する」とする警告もある。ほとんどは、ペットの癒し効果とか、迷信として片付けられてきた。しかし、この2~3年、欧米の研究者からネコのもつ不思議な力の源泉が、病原体の原虫にあるのでは、とする説が提唱されるようになった。
もしもの備えは万全ですか 保険は、住宅に次いで高い買い物
ーーーーー
昨年10月末に開かれた衆議院の財務金融委員会。質問に立った自民党のあべ俊子議員は、中塚一宏金融担当副大臣を問いただした。医療保険の募集広告があまりに誇大で、消費者の誤解を招いているのではないかとの趣旨だった。
こういう側面もあるのかもしれない
不思議な王子
ガラスの靴で確認するという仕組みである
第一足のサイズが同じ程度というのは
特異性が低すぎる
第二、足のサイズを確認しないと本人かどうかわからないというのは
王子はなにか部分的に不自由なところでもあったものだろうか
シンデレラとしては、ガラスの靴で本人確認をしないといけないような王子様だと
ちょっと考えるのではないか
第三、こんな事言ってもぶち壊しなんだけど
王子もシンデレラも何に惚れたのか全くわからない
そのあたりからの派生で
ガラスの靴というのはヴァギナのことで
暗闇の中での相手不詳のセックスが良かったけれども
それが忘れられないので探せという命令になり
しかたがないので片っ端からセックスをして確認していったというバージョンもあり
ガラスの靴とぴったり合う足をした女性
というのはつまりはそういうメタファーなのだそうだ
いや、普通に考えると
暗闇でのセックスが良かった女性よりも
昼に笑顔の明るい女性がいいように思うけれども
どうなんだろう
王子は、いろいろと探し歩いているうちに、
ガラスの靴にはぴったりではないけれども、
この人が好きだなと思うような女性はいなかったのだろうか
不思議な王子である
排卵日に殿を独占する
排卵のある女性が集団で暮らしていると
ある程度排卵日が一致してくる
平安貴族とか江戸大奥とかがそんなものだろう
すると、お世継ぎをうまく産み落とすには
排卵日に殿が来てくれることが大切で
排卵日以外は別のところに行ってくれていてもいいわけだ
しかし排卵日だけは独占しないと
自分が妊娠しないし他の女性に妊娠されてしまうかもしれない
ボスが多数の女性を独占するように見えて
実質は排卵日の独占だけが問題なのだろう
昔のことだから月の満ち欠けと
月経現象が同期して考えられていたはずで
だから月は今よりずっと大切だっただろう
よく知らないが満月の日とかはいろいろしそうな気がする
ーーーーー
排卵日以外でも妊娠しますという方法もいくつか知られていて
お世継ぎを懐妊するならそれでも良かったはずだと思う
ーーーーー
姫よりも殿が欲しかったはずだけれども
そこの辺のデータは乏しいような気がする
成人前に死んでしまう子が多かったから
よくわからないのかもしれない

メールでの誤解
実際にあって話すと誤解が起こったとしても+-20程度とすると
電話で話した場合は+-50くらい
メールで連絡した場合には+-100くらいだろうと思う
怒っているけれど、本当は許したいんだとか
そのあたりがなかなか伝わらないのだろうと思う
Psychopharmacology under the microscope
翻訳語
たとえばoftenをいつもしばしばと訳すのは芸がないので
いろいろと場面に応じて訳し分けたりするのだけれども
考えなおしてみて
oftenはいつでもしばしばと決めてしまえば
読者はしばしばを日本語の意味で解釈しないで
これは英語のoftenと解釈すれば
とても便利なのだと思った
オフンと訳してももいいのだと思う
そんな日本語は嫌だというならそれもいいけれど
しばしばとは頻度が高いことで、などと考えていないで
このしばしばは英語のoftenの意味だなと思うことで
充分なのではないかと思う
ぴったりの日本語がないときに造語して何かの言葉を充てたりするのも
言語を思い出させるのでそれは誤解のない方法だと思う
既存の日本語だと、初学者の場合、その日本語の意味に引きずられることもあるだろう
勉強している人は、この言葉は英語のあれだなと見当がつく
agitation などと言う言葉では
辞書では不穏、興奮、焦燥などといろいろと載っているのだが
激越と訳すと、これはagitation depression のときの言葉だなと見当がつく
激越を鎮めるといえばうつ病なのに興奮しているという奇妙な、一種の混合状態を
鎮めるという意味で
単に不穏でもないし興奮でもない
不穏や興奮は、シゾフレニーでもパニック障害でも認知症でも起こる、一般的な語彙である
激越というだけでそれはagitationのことでしかもdepressionのときの言葉と
だいたい決まっているので話が早い
しかしその事は日本語辞書にはないだろうし
漢字の意味をたどっても分からないと思う
広汎性とpervasiveの関係もそんなものだろう
広汎性の文字から何かを分かろうとしても不正確な話でpervasiveのことだと
一旦理解して、そこからだろう
便利といえば便利なのだが
初心者がささっと理解するには少し不便だろう
今後この方面で仕事をするというのでもなければ
ささっと理解して、結局どうすればいいのかを知ればいいように思う
そんな場合に、このような翻訳後のメカニズムなどは必要なのだと思う
たとえば批判という言葉があるが
これはカントの場合はKritikのことで
別に非難することではなくて、厳密に考えるという意味だけれども
カントの文脈で批判というとクリティークの意味でというのは
業界の決まりになっているので
批判的意見と好意的意見の対比としての批判ではないのだと
分かる仕組みになっている
純粋理性批判といっても純粋理性を悪く言っているのではなくて
純粋理性というものについて厳密に考えてみるという意味で
それを昔から批判という日本語を充てる習慣になっているというだけである
なにか日常用語としては決して使わないような言葉を充てるのも方法だったような気もする
しかし一般初心者が誤解するとしても最初から挫けてしまわないようにする働きもあるのだと思う
たいていとしばしばと頻繁にとよくあることだがと多くの場合と
日本語としても差があるように思うが
その言葉の網の目と
英語のoftenとかfrequentryとかalwaysとかmostlyとかの
意味の分担の網の目は違うのだろうから
そのあたりもややこしい
性格障害、人格障害、のあたりもパーソナリィ障害でまとめようというらしい
性格異常とか人格異常はまたなにか違う意味のにじみがあるようだ
シゾフレニーという言葉は
どこの国でも変化なく使っているのに
日本でだけ用語の変更があって
すると検索の場合とかで不都合が生じる
シゾフレニーを多重人格と混同しているのは日本だけではなくて
アメリカでもイギリスでもあるようで
混同しないようにと啓蒙書には記述がある
疾病と障害の違いは大切なのだが
disease、disorder、impairment と並べると
やはり言葉の網の目の違いを感じる
ーーーーー
漢字には歴史があり
歴代の王朝で読み方が違い
意味も違うことがある
同じように現代の日本語の言葉を英語の何かの単語に強く結びつけて
意味を拡張することも行われていいことなのではないかと思う
メールの言葉
出来れば電話で話したいし
一番いいのは実際に会って
顔を見て話したいのだという
何が不満かというと
メールでは言葉がただの素っ気ない言葉になっていて
実際に話すときの色合いとか深みとか微妙なところが伝えられなくて
もどかしくてダメなのだとのことだ
MIDI音楽という変なものがあって
だいたい分かるけれども
あまり感動はしない
それと実際の歌との違いくらいのことを
その人はメールと会話の間に感じているらしい
ーーー
言葉の背景にあるコンテクストというものを読み取れない人がいるもので
これも実に興味深いことだと思う
「はい」と答えて、そのままイエスのこともあるし、思いっきりノーのこともあるし
ただ単に「はい」という言葉が投げ出されているのでは
何もわからないと感じる人もいるらしい
逆に「はい」は肯定なのだから、それでいいという人もいる
私として不思議なのは、こんなにも解釈の違う人間が
同じような場所に生きていて
別に不都合もなく生活は進行しているということだ
カラーと白黒くらい違うけれども
それはそれで他人の心の中には踏み込まないで
生きられるものなのだと思う
Y遺伝子
A家男子YXとして
B家女子X1X2として
女子が生まれると
XX1またはXX2
たとえばXX1が後継になったとして
その配偶者が
C家の男子Y3X3とすると
女子が産まれたとしてX1X3の可能性があり
その女性はB家とC家の子孫ではあるが
A家の子孫とは言いにくいような気がする
つまり3代でA家はB家とC家に乗っ取られる可能性がある
という話をされて、まあ、どうでもいいが、そうかもしれない
XXの間で部分的な交換もあるのだろうからそんなに100%の話でもないのかもしれない
それもよく分からない
実際の話は
男子は子供が自分の子なのかどうか怪しい
しかし数多く残せるので
昔のように子供がたくさん死ぬような環境だと
男子のほうが効率良く遺伝子を残せたかもしれない
しかし誰の子なのかという問題は解決されない
しかしそれを利用して水増しもできる
女子は自分の子であることは確実なのだろうが
数が確保できない
死ぬ確率が高いと女子の相続は不利になる
ところが自分の子であることは確実とは言いながら
生後に取り替えられたりすることはいくらでもあるだろうから
男子ほど怪しくはないとしてもやはりなんとも言えないだろう
昔の人はY遺伝子の話など知らないはずなので
別の理由で決めたものなのだろうし
歴史は現在の都合で作られているものらしいので
ますますよく分からない
2の累乗の計算をしてみるとあっという間に膨大な数字になるので
たとえば20歳で子供を産むとしてみても
あっという間に日本人全部の家系が重複してしまう
一人何役もする以外にないらしい
ーーーーー
昔の話をすれば
生年月日がはっきりしているのは最近になってからのことではないだろうか
記録係がいるような家庭ならば別だが
一般家庭では年齢など曖昧なものだろう
だから若く見えれば若いと判断されたはずだろう
そんなあたり、年齢不詳の世界で面白い
だから妊娠を確認してから入籍などの習慣もあったようだ
若者は幸せである Happiness is circle Knowledge is ellipse
ものを知らないから幸せでいられる
そして将来、知れば幸せになるかもしれないと希望することができるから
老人は不幸である
ものを知ることで不幸であり
不完全にしか知りえないことで二重に不幸である
ーーーーー
若者は幸せである
知らないから
老人は二重に不幸である
知るから
そしてそれが不完全であるから
幸福は円であるが
知識は楕円である
あるいは完成しない円である
they believe they will know something and become happy
Happiness is circle
Knowledge is ellipse or incomplete circle
フリーズドライ精子
文学とは何か
言葉というものは体験や思考を自分のために書き留めたり
他人に理解してもらうために書いたりなど
実用的な側面があり
その端的な例は法律とか命令とかそんなものだろうが
その対極的な言語の使命として
言語は何を語り得るか何を語りえないか
そして言語で語りえない世界をなおも語る試みというものが
長い間続けられてきている
それが言語の歴史であると思う
言語の生成を考えてみると
言語が出来る前に思考は明確にはなかったかもしれない
言語が生成されて思考が成立した
認識が成立した
しかしそれは狭い範囲であった
語彙も少なかった
それが次第に語彙を増やし
メタファーを増やし
語り得ることと語り得ないこととの境界を乗り越えて拡張していった
それが同時に人間の認識世界の拡大でもあった
それは現在でも進行していて
言葉は日々新しく作ら入れているし
外来語の正しい用法もあり誤用もあり
それらすべてを含めて言語世界が、非言語世界を侵食するプロセスである
言語が成立してどれだけ年月が経ったのか正確にはわからないが
それでも未だに言語の外側に壮大な世界が広がっているようである
そして今もなお、日々新しく、昨日までは語り得なかったことを
語り得ることに変更しつつある
それにしてもいつまでも語り得ないいことが
言葉の外側にあるのはどうしてなのだろう
一見すると、語り得ることと認識し得ることは一致していて
語り得ないことは認識し得ないことと考えられるのだが
人間はいつも語り得ないことを感じていて
それを言語世界に変換することに挑み続けているのである
なぜいつでも常に語り得ないことが広がっているのだろう
語り得ることについては語り得た
だからこれから以降、言語の新作もないし、メタファーの新作も必要がない、
そう宣言しても悪くないくらいの歴史だろうと思う
それでも停止せずに常に運動を続けている
それが文学の営みである
すでに共有された言葉で、すでに共有された世界を退屈しのぎに描くことは
消費される娯楽ではあるが
語り得ないことを語り得ることに変換するという
私の定義する文学ではない
私は個人的には言語の拡張的な使用法を試みているつもりである
地熱発電と噴火
火山が噴火する可能性を考えると
結構大変かも
高知県など海の近くは危ないというので
山に登ると今度は噴火が怖い感じはする
何しろ地殻変動が激しいのだから
ーーー
いろいろなデータが出されるたびに
不動産の値段が変動する感じはある
ーーー
どこに逃げても困るだろうなと思いつつ
しかし見方を変えれば
自然が日本人を根絶やしにすることはできないだろうと思う
日本全部が沈没すれば、海外にいる日本人を別にして
日本人全滅だろうが
そうでもなければ
どこかの部分は生き残るだろうから
どの人が生き残るのかは分からないけれども
誰かが生き延びるだろう
集団生存とか集団遺伝学としては、それだけで充分なのだろう
防災設備にどれだけのお金をかけるかという点で言えば
実際難しいところがある
1000年に一度の災害のためにどれだけのお金をかけるのかは
冷静に考えないと
工事を請け負った業者が、どうせ1000年後にしか使わないのだから
手抜き・中抜きでもいいと考えないとも限らない
工事の結果として災害に耐えられるのかどうかを検証するのは難しい
壊れるまで実験しないと分からないところがあるだろう
非破壊的な検査でどこまで分かるか、謎がある
この場面でも、悪徳業者の暗躍が予想される
一時問題になった耐震偽装問題はもう解決されたのだろうか
ーーー
だってふるさとはアフリカだからなと言い出しかねない
満開の人生の景色
満開の桜の下を歩いて通勤した
桜満開、春、若者、新年度、お酒、出会い、希望、期待、ここまでそろっても
憂うつだというのは大伴家持くらいのものだろう
満開の花が過ぎたあとはもちろん寂しい
しかしだからといって満開の花を見たくないのではない
これが人生の景色なのである
躁病になって自分も大変な目にあい周囲にも迷惑をかけ
友人を失い職を失い
それはもちろん大変なのだけれども
それが人生だという気もする
この満開の花を見ると
そう思う
躁病が満開の花だというのではないが
人生にはいろいろな景色があるものだという思いがある
人生の中で何度か躁病にもなり何度かうつ病にもなり
そのようにして人生の景色が刻まれて
思い出が残る
それでいいような気もする
それで大きな損失が出るとしても
それが人生だろう
死んでしまったあとで平和な人生だったなあと思うのと
起伏のある人生だったなあと思うのと
どちらが悪いとも言えないような気がする
bipolar vs monopolar
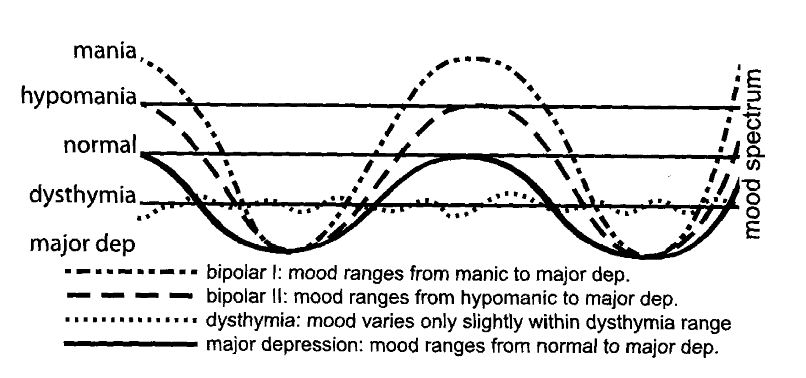
この図を再掲するのだが
この図を見てnormalがゼロでmaniaが+、depressionが-とは
私には見えない
磁石のようにNとSが混ざっているとかも見えない
maior depression のラインがベースラインで
maniaが100とすれば、hypomaniaが75、normalが50、dysthymiaが25、
major depressionが0としか見えない
すると2つの因子を仮定する必要は全くなくて
因子としては1つなのだろうと思う
それが50くらいのときに、人間としては普通くらいの感じということなんだろう
上記のライン以外にも組み合わせとしては無限のバリエーションがあるのだと思うが
それは病気としてわざわざ認定する必要がないからなのだと思う
major depressionで職業的、社交的に機能停止してしまうので一番不都合ということなのだろうと思う
不都合というのは社会にとってが半分で本人にとってが半分
bipolarという呼び方もおかしくて
私にはmonopolarにしか見えない
mania成分が0-100の間で変動しているだけと見える
二極があるといってもこれでは一極なのである
たとえば、セロトニンとノルアドレナリンの量が独立に変動して
二極の合成として示されるというならば
双極性と言う言葉がふさわしい
しかしその場合には
うつの軸とそうの軸を直交させて描いたほうが分かりやすいだろう
そのような書き方がふさわしくないというならば
やはり一極で
変動要素は1つだけなのである
直交させるのが分かりにくいなら
時間軸を横にして
うつとそうの成分をそれぞれ独立にグラフにすれば分かりやすいだろう
そもそも混合状態の時にはそのような書き方をすることもあるのだが
混合状態に関しても、そうが100と25で混じるから混合状態というだけだろう
英語は90点で数学が20点なら混合状態となるのだろう
しかしそんなことはいくらでもある
この話はずっと昔からある話で特段に新しい話でもないのだが
最近はあまり言われないようだと感じている
その昔からの説で言うと
depressionになるのはmaniaがあるからである
maniaがずっと続くはずはないので
いつかは低下する
低下した時が0になるとdepressionで50になるとnoramalということで
たとえば子供の場合には50-100の間くらいで変動していると思う
成人に近くなってmania細胞がそれなりに年をとると
depression phase が始まるのだろう
人によってはmaniaまで上昇しなくても
normalのあたりで活動していてもmania cell にダメージが生じて活動停止になることがある
それが単極性うつ病に見えるということになる
遺伝的に双極性障害と単極性うつ病は分離できそうだという話も当然で
mania cell の分布は遺伝的に規定されているので
mania cell の性質と量によって単極性に近いか双極性に近いかが決まるのだと思う
お祭り騒ぎが好きな一家とそうでない一家があるというだけのような気がする
それぞれで大うつ病は経験する
その場合、単極性うつ病一族はもともとmania cell が少ないと興奮しないのだから
抗うつ剤を投与しても躁転することもない
極点に言えばうつ病で自殺したり
躁病でお金を使い果たしたりしない限りは
昔と同じく放置しておいても元に戻るので
積極的に薬剤を使用する理由がないといけない
薬剤使用の利益が明確でないといけない
もともと循環性で元に戻るものと定義されていたのだから
反復はするがレベルダウンはしないのである
それを、実はレベルダウンがありますというなら、
かなりの大変更なのである
そして多分実態はレベルダウンがある
昔からそう言われてきていたが
ドイツ精神医学の建前上は一応レベルダウンがないこととして
純粋理念型を立てるということになっていた
なにしろ人間は長生きするようになったし
そのなかで高度情報化されて仕事をしていて
わずかのレベルダウンも敏感に拾い上げる社会構造になっているのだ
だから50年前に比較すると
明らかに個人の機能レベルダウンは把握されやすくなっているし問題になりやすくなっている
そんな背景があるので
躁うつ病にもレベルダウンがあるという話になっている
しかしこのレベルダウンとシゾフレニーでのレベルダウンは
やはり様子が違うだろうと思う
てんかんも含めて、人格水準の低下という点では似ているものなのだけれども
気分障害の場合には顕著ではない
ーーーーー
mania細胞がフル活動している100のとき、人間として最高の能力を発揮するかといえば
必ずしもそうではない
たとえば本を書くという一面的能力ではそう状態のときに有利かもしれないが
その状態で他人に尊敬される、自分で後から思い返してみて誇らしい、
そういう状態ではないだろうと思う
妙に仕事ははかどったけれども、やっぱり病的だったな、という感想だろうと思う
人格水準低下という曖昧な言葉を使うのだけれども
高位脳機能の障害された状態である
その状態のままで普通に行きている人もいくらもいるので
あまり深刻ではないし
幸せになることを考えると、その事自体はあまり障害にはならないのではないかと思う
Atypical Antipsychotic Drugs and Alzheimer's Disease
Smoking and Mental Illness — Breaking the Link
Genomics, Intellectual Disability, and Autism
Adjunctive Antidepressant Treatment for Bipolar Depression
androgen-deprivation therapy can cause major depression
自分撮り take a picture of yourself instead of writing a diary
現在であれば、例えば、朝身支度をして出かけようとするときに
自分の姿を写真にとって
自分の身繕いとか表情を確認するという方法も
悪くないのではないかと思う
ーーーーー
SmaPG理論
最近いくつかまとめたので
参考に
smapgはスマップ・ジーと読んで、
Stress Management Power Group の略です。わたしたちのことです。
『こころの科学』 ネット社会とこころの悩みとDAM理論 今 忠 2009
http://shinbashi-ssn.blog.so-net.ne.jp/2009-05-21
英文 My Original Theory-1 DAM Theory in English (Depressive-Anankastic-Manic Cells Theory :Conprehensive biological theory for manic depressive disorder ,mood disorder and premorbid character traits)
http://shinagawasn.blog.so-net.ne.jp/2011-10-18-1
英文 My Original Theory-2: Pathological Hypothesis of Schizophrenia:
First/Second World Model, Time-delay Hypothesis,Temporal profiles of Neurons
躁状態先行仮説:気分障害再考
http://shinagawasn.blog.so-net.ne.jp/2011-07-17-1
「統合失調症とうつ」
イメージ空間測定法
自我障害の話 smapg-time-delay model
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-04
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-09-1
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-06-4
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-06-11
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-12
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-6
山内名誉教授の左右脳のお話
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-17
シンメトリーの話
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-23
その手前までの基本的な話
http://shinbashi-ssn.blog.so-net.ne.jp/2007-11-25-3
躁うつ病 smapg MAD-theory
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-04-23
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-13
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-4
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-5
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-2
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-1
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-14-11
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-14-6
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-14-2
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-14-1
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-14
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-13-3
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-19-5
統合失調症リハビリについて
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-07
うつのリハビリについて
ドパミンレセプターとセロトニンレセプター
セロトニントランスポーターと幼児期別離体験と牛若丸
体質改善のメカニズム
ネット社会とこころの悩みとDAM理論
http://shinbashi-ssn.blog.so-net.ne.jp/2009-05-21
精神療法について
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-12-1
山内教授のうつのお話
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-6
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-1
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-2
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-3
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-4
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-5
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-6
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-16-7
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-29
うつの治療
http://shinbashi-ssn.blog.so-net.ne.jp/2008-06-05
種々の新型うつ病についての並列的概観
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15
種々の新型うつ病と病前性格についての導入
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-15-1
ディスチミアの説明
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-3
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-4
不安の病理と治療
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-19-4
認知療法的領域
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-19-3
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-25
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-26-2
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-26-4
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-1
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-2
食べ吐き
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-28-7
嗜癖
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-30-1
感覚の能動性と脱能動性
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-30-3
中心感覚と辺縁感覚
http://shinbashi-ssn.blog.so-net.ne.jp/2008-05-30-4
ハリネズミのたとえ
http://shinagawa-lunch.blog.so-net.ne.jp/2010-12-03-7
アンビバレントの汎化
http://shinagawa-lunch.blog.so-net.ne.jp/2011-02-13-8
SMaPG式性格類型の提唱
http://shinagawa-lunch.blog.so-net.ne.jp/2010-11-25-14
My Original Theory-2: Pathological Hypothesis of Schizophrenia: First/Second World Model, Time-delay Hypothesis, Temporal profiles of Neurons
the therapeutical effect of cognitive-behavioral therapy
My Original Theory-1 DAM Theory in English (Depressive-Anankastic-Manic Cells Theory :Conprehensive biological theory for manic depressive disorder ,mood disorder and premorbid character traits)
My Original Theory-1
DAM Theory (Depressive-Anankastic-Manic Cells Theory :Conprehensive biological theory for manic depressive disorder ,mood disorder and premorbid character traits)
Tadashi Kon(Shinagawa Psychosomatic medicine Clinic)
〒108-0075 2-14-10-10F Kounan,Minato-Ku,Tokyo,Japan
1. DAM Cells :Enthusiasm, regularity and the persistence of negative mood are biological indexes
When we assume chronic continued stress to a neuron, three types of neurons are predictable according to the responses to the repeated stimulation.
First, there are neurons whose reaction speed gets gradually faster, such as neurologic kindling (epilepsy) and hysteresis (schizophrenia). I call these types of neurons M (Manic) neurons as they relate to the manic state. They also relate to enthusiasm, excitement (hyperthymia), and energy.
Secondly, there are neurons that always react steadily to the repeated stimulation.
I call these types of neurons A (Anankastic) neurons. A neurons are an element of regularity.
Thirdly, there are neurons whose response to the repeated stimulation rapidly diminishes. I call these types of neurons D (Depressive) neurons because they relate to the duration and weakness of the negative mood. The majority of the human brain neurons are considered to be this D type.
2. DAM Theory : the onset mechanism of depression
When M neurons respond more and more actively to the recurrent sustained stress, the body is in a manic state. When M neurons burn out and stop functioning, D neuron traits emerges, and the body is now in a state of depression. Once M neurons recover from the damage after a sufficient interval, they restart their activities and become in a manic state again. Repetition of this procedure creates symptoms of bipolar disorders. I think that depression doesn’t exist alone. It is always accompanied by a manic state where M neurons are activated, at least immediately before the depression, no matter how subtle the manic state is. The obsession element of A neurons appears and disappears because the obsession comes to the foreground and recedes into the background according to the state of bipolar disorder. When M neurons cease to function and A-type neurons are enough in number, the obsession comes to the foreground instead of depression. If we assume that M neurons are related to circadian rhythm, insomnia and diurnal change (depressive mood and inhibition are strongest in the early morning and remit in the afternoon to the evening) are explained by the lack of M neurons’ element.
3. Explanation of Premorbid Character
Quantity and distribution of M, A, and D neurons in the brain explain part of premorbid characters. Intermediate types of the three types will exist and they construct a continuous spectrum.
(1) Brains with high M neuron elements are enthusiastic, having characters of bipolar and cyclothymia. BP (Bipolar mood disorder) Ⅰ and Ⅱ belong to this type. BPⅠ consists of a manic state and depressive mood; BPⅡ consists of a hypomanic state and depressive mood. One affected by bipolar disorder with a premorbid character as cycothymia belongs to this type. The immature form of depression is for immature and narcissistic cyclothymia, and is usually an early-onset type. It is difficult to distinguish the immature form of depression from personality disorders. Avoidant depression is also close to this type.
When the society itself is in a hypomanic state, that of BPⅡwill be hidden. From the Meiji era to the high economic growth period, BPⅡ were diagnosed as single episodes of major depressive disorder. Madness towards the war and the devotion to company organizations probably belonged to a hypomanic state. Good adaptation often turns out to be a hypomanic state.
(2) Brains with significantly more A neuron elements than M neuron elements are regular and have strong compulsive elements. Typus melancholicus, premorbid character of melancholic type depression, belongs to this type. While A neurons are responding to repeated stimulations, compulsive tendencies are presented. After A neurons get too tired, they cease to function. At that time, usually, M neurons are also too tired and resting, and they are in a depressive mood. If M neurons recover quickly, mixed episodes of manic-depressive are shown. Retreat neurosis is close to this type.
Tardy and nonchronic type of atypical depression is close to the melancholic type. Premorbid character of juvenile-onset chronic type of depression has not been clearly explained yet. Beard type depression is said to occur in the narcissistic immature type character when the office (workplace) is melancholic (where perfection is required of workers).
(3) Brains with relatively few M neuron elements and A neuron elements possess weak characters without strong enthusiasm nor regularity. People with modern weak characters have lost self-confidence superficially, but mostly hold on to exaggerated egos inside them. Sometimes exposure of that exaggerated ego is observed. That is, it is not a unilateral weakness, and it strongly possesses a narcissistic element most of the time. It is a combination of weakness and immature narcissism. When it becomes depression, one may call it an immature narcissistic type of weak character type depression. However in DSM it is close to dysthymic disorder(long lasting mild depressive tendency) as the symptom of the first, Ⅰ axis, and it is close to dysthymia-affinity-depression among modern types of depression.
(4) Brains with plenty of M neuron elements and A neuron elements show immodithymic characters with strong enthusiasm and regularity. According to the temporal profile of functional breakdown and recovery of both elements, manic, depressive, mixed episodes of manic-depressive, and further mixed episodes with compulsive tendency are observed. It is difficult to distinguish from personality disorders, if one onsets around 20 years old.


